Acta Medica Scandinavica. Vol. 178, fasc. 2, 1965
From the Department of Medicine, Karolinska Institutet, at
Serafimerlasarettet, Stockholm, Sweden
On the Relationship Between Water Hardness and Death Rate
in Cardiovascular Diseases
By
GUNNAR BJÖRCK, HARRY BOSTRÖM and ANDERS
WIDSTRÖM
Read before the European Congress of Cardiology in Prague,
August 1964
The marked geographic variation in the distribution of
cardiovascular diseases is well-known and often emphasized (4,
10, 11). It has been the impetus to many studies on the possible
influence of various environmental factors. One of these factors
is the chemical composition of drinking water. Thus,
epidemiologic investigations in Japan, the United States and
Great Britain have indicated a higher death rate from
cerebrovascular and cardiovascular diseases in areas with soft
water than in hard water regions (1, 3, 5, 7, 9, 12, 13, 14).
High sulphate concentration in the river water in Japan (5, 12)
has also been positively correlated to death rate in
cerebrovascular disease. In some studies, however, no correlation
has been found (6, 8). The matter has been discussed by Schroeder
(15), Dingle et al. (2) and others. Gastric cancer has been found
more commonly in areas where the water is soft and has a low pH
(16). In the present paper we will briefly report on results
obtained from Sweden.
Material
The study is based on material from all Swedish towns with
more than 25,000 inhabitants, 33 in number, and in addition Visby
on the island of Gotland. The distribution within the country is
seen in fig. 1, in which also
areas with primitive rocks (white) and sedimentary rocks (shaded)
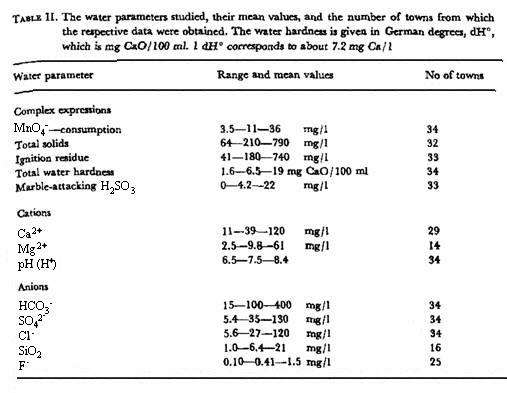
are indicated in table I
information is given for each town about number of inhabitants,
geology, type of water source and some chemical parameters in
drinking water as supplied.
From the local water-works we have obtained the available
annual mean values for 23 chemical analyses of the finished
drinking water supply from 1940 to 1962. Sixteen of these
analyses on at least 1 sample a year are required by law for all
works. The period thus covered varies from 5 to 24 years (mean
16), the number of samples subjected to routine analyses from 1
to about 50 a year. Some parameters have been excluded because
the values are near or below the limit of the analytical method
or because they have been determined at too few works. The
remaining water parameters are listed in table II.
From Statistiska Centralbyrån, Stockholm, we have
obtained the number of inhabitants in the censuses 1950 and 1960,
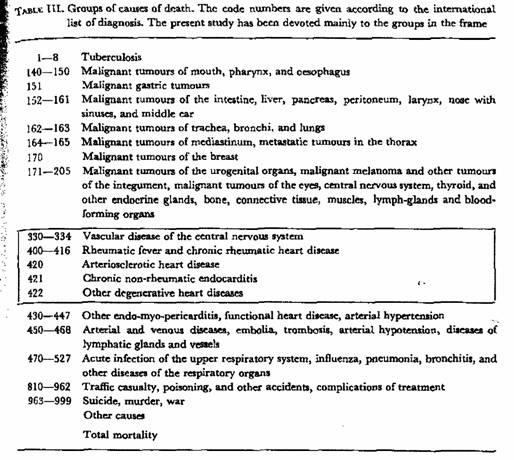
the absolute number of deaths from 19 specific groups of causes
and from all causes, for both sexes and the age groups
25—44, 45—64 and 65—74 years separately, for
each year during the period 1951—60 in the respective
towns, and the mean age-adjusted death rate for the period. The
groups of diagnoses are given in table III.
Methods
1. Correlations between the various water parameters, and
between death rates from various causes and each of the water
parameters, were calculated with the aid of a computer.
2. For the age group 25—74 years the death rates from
causes 420 and 422 were plotted separately as well as jointly
versus total water hardness and concentration of Ca2+. The
equations of the corresponding regression lines and the
significance of the slope (t-coefficients) were calculated.
3. For the age groups and sexes separately, multiple
regression analyses of the death rate from causes 420 and 422
versus six water parameters which were considered to have little
interdependence, were made in unselected order with a
computer.
4. The ratios of death rates from causes 420/422 were
calculated for the 3 largest cities for each year during the
period, from the absolute number of deaths in the age group
25—74 years. The same ratios were also calculated for 9
towns with a mean water hardness less than 3 mg CaO/l00 ml and 6
towns with more than 14 mg CaO/l00 ml.
5. The mean death rates from cause 422 were calculated for the
periods 1950—55 and 1956—60 and correlated to the
mean concentration of Ca2+ for the whole period. The 10-year mean
number of inhabitants was, an approximation taken to be the value
for 1955.
6. The death rates from causes 420 and 422 in Stockholm for
each year were calculated after interpolation of the number of
inhabitants between censuses undertaken in 1950, 1955 and
l960.
In the tables the following symbols for the degree of
significance will be used: * = probably significant, p < 0.05;
** = significant, p < 0.01; *** = highly significant, p <
0.005.
Results
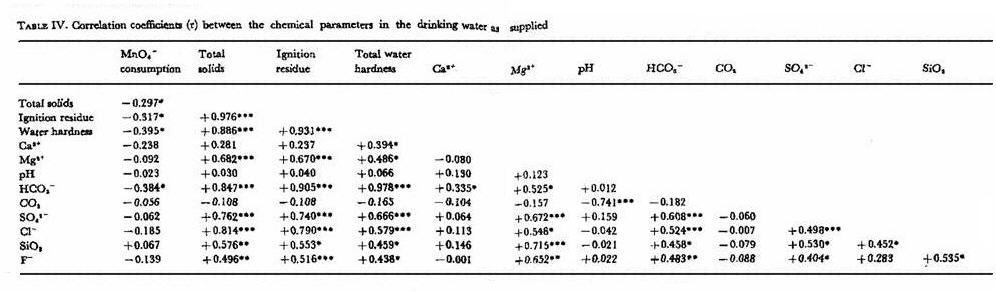
The correlation between the various water parameters is
indicated in table IV.
Evidently, there is a large group of water parameters varying
together; total solids, ignition residue, total water hardness,
concentrations of Mg2++, HCO3-, SO42-, Cl-, SiO2, and F-. The
concentration of Ca2+ is correlated to total water hardness and
concentration of HCO3-, but not significantly related to other
factors, MnO4-consumption, an expression of the amount of
reducing substances (mainly organic) in the water, tends to vary
inversely with the large group of inorganic constituents
mentioned above. The pH is significantly correlated only to the
concentration of marble-attacking HCO3-.
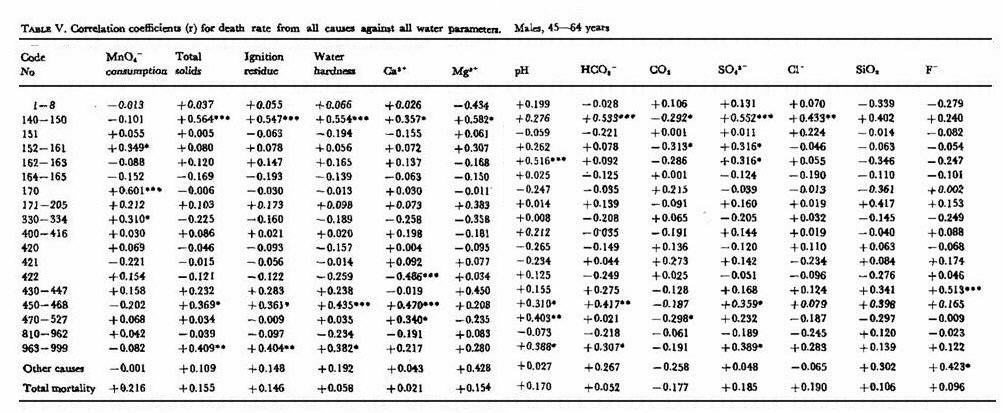
The results of the correlation between death rates and water
parameters (r coefficients) are summarized in table V (males) and table VI (females). Total mortality
— death rates from causes not here specified as well as
from most of the specified causes — were not significantly
related to any of the water parameters. For certain groups of
causes, however, e. g. malignant tumours of the upper digestive
tract (140—150), vascular diseases (450—468) in the
males, and breast cancer (170) in the females, highly significant
positive correlations to the inorganic group of water parameters
were found (p <0.005). For death rate from cerebrovascular
diseases in the females, a probably significant negative
correlation was found to the same group of water parameters (p
< 0.05). The concentration of Ca was significantly negatively
correlated to the death rate from “other degenerative heart
diseases” (422) both in males and females. Similar patterns
were to some extent obtained in the other age groups.
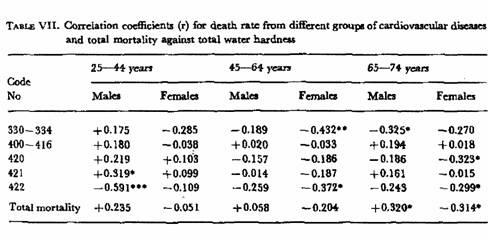
In the present investigation only the group of cerebrovascular
and cardiovascular diseases was studied in some detail. Table VII summarizes the correlation
(r-coefficients) to water hardness for all the sex- and age
groups. In the youngest male group a highly significant negative
correlation (p < 0.005) for water hardness was found with
“other degenerative heart diseases” (422), mainly
so-called “cardiosclerosis” or “myocardial
degeneration”. A significantly negative correlation (p
<0.01) was found for cerebrovascular diseases in the middle
age group of women. In addition, scattered significances at the p
< 0.05 level were seen.
Table VIII shows the
correlation coefficients (r) for the death rates from these
cerebrovascular and cardiovascular diseases to the concentration
of Ca2+. For males a highly significant negative correlation was
found to the group of “other degenerative heart
diseases” (422) in all age groups (p <0.005). In the
females a corresponding correlation increasing with age was
noticed: in age group 45—64 years p <0.01, and in the
group 65—74 years p <0.005. For none of the sex- and age
groups was any correlation found between death rate from
arteriosclerotic heart disease (420) and concentration of
Ca2+.
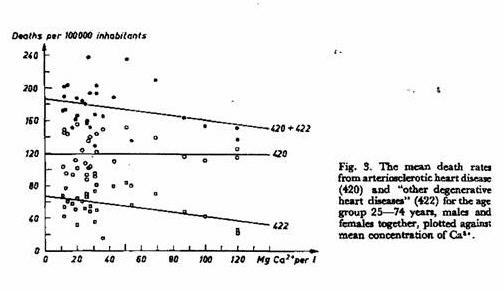
The same relation is illustrated in figs. 2 and 3. The death rates from
arteriosclerotic heart disease (420) and “other
degenerative heart diseases” (422) for the age group
25—74 years, both sexes together, were plotted against
total water hardness and concentration of Ca2+ respectively. The
slopes of the calculated regression lines are highly significant
(p <0.005) for 422 against both water parameters and
significant (p <0.01) for 420 against water hardness, but not
against concentration of Ca2+.
The multiple regression analysis showed no significant
correlation between any of the water parameters
(MnO4-consumption, concentrations of Ca2+, HCO3-, SO42, Cl-, and
pH) and death rate from cause 420, with the exception of
concentration HCO3- in the youngest males. The death rate from
cause 422 was found to be significantly correlated to
concentration of Ca2+ in all the male groups, and in the youngest
group also to Cl- and pH. For the females the death from cause
422 was significantly correlated to pH and concentration of Ca2+
in the middle age group, and to the concentration of HCO3- in the
oldest.
These rather startling findings forced us to analyze the group
“other degenerative heart diseases” in greater
detail.
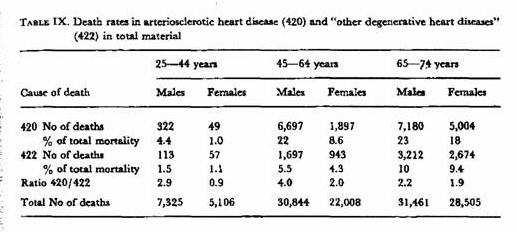
Table IX shows the actual
number and the number as a percentage total mortality, of
patients in the various age groups and sexes whose causes of
death were registered as arteriosclerotic heart disease and
“other degenerative heart diseases”, respectively. On
an average the ratio of the diagnoses 420 : 422 in males is 3 :
1, whereas in females it is closer to 3 : 2.
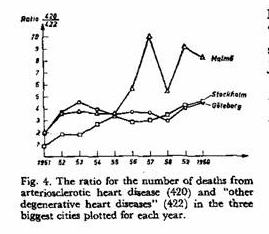
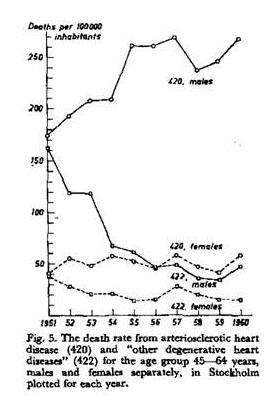
There is, however, a strong tendency in later years towards an
increased assignment of 420 in preference to 422. This fact is
indicated in figs- 4 and
5. The ratio for the number of
deaths from 420/422 in the three biggest cities shows a three- to
fourfold increase during the 10-year period, as seen in fig. 4. The plot of the death rate
from causes 420 and 422 in Stockholm shows ( fig. 5) that the change in the
assignment of the diagnosis numbers refers mainly to the
males.
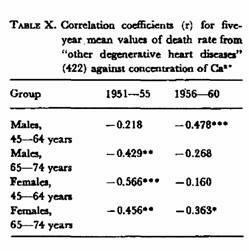
In view of this tendency, it seemed worth while to analyze
whether the correlation of mortality from No 422 to low calcium
concentration was more marked in the beginning or at the end of
the period studied. The results are given in table X. This table substantiates the
over-all negative correlation, but unfortunately does not give a
definite answer to the said question. Farther studies, therefore,
are necessary on this point.
Discussion
The results presented in a general sense agree with those
published from Japan, U.S. and England (5, 7, 12, 13, 14). Once
more, in still another part of the world, in a country with a
very homogeneous and stationary population, which is reasonably
well organized as far as population statistics and water supply
are concerned, the very strange fact has been revealed that
“water hardness” and some constituents of drinking
water associated with water hardness are in one way or another
correlated to a specific fraction of the death rate in
cardiovascular diseases.
The interpretation of this fact has been discussed in some
detail by earlier investigators, and various suggestions e.g.
concerning the possible role of certain trace elements deriving
from soil or water pipes etc., have been made.
We have great difficulty in explaining why the calcium
concentration in water should affect cardiovascular mortality,
when the relationship between calcium content of water and of
food is considered. It appears to us most reasonable to regard
calcium as an “indicator” of something else, which
might be a causal agent. Trace metals may be one type of factor
that could be operating. Other environmental factors might also
play a role. These problems will require further study.
Another aspect which has been brought out by this study is the
question of the homogeneity of the statistical group 422 -
“other degenerative heart diseases”. This group has
long been regarded as a waste-paper basket into which doubtful
and difficult diagnostic problems were thrown. Patients not
suffering from clear-cut angina pectoris or myocardial
infarction, but eventually dying unexpectedly or with heart
failure in the absence of valvular heart disease or hypertension,
have been referred to this group. Recent puritanism in the
diagnostic nomenclature has caused a gradual giving up of that
diagnosis in preference to 420 — arteriosclerotic heart
disease. And now it turns out that — whatever the causal
relationship involved may be — this group 422 repeatedly
shows homogeneity in this statistical analysis of fairly large
numbers. This is true of our study, but it is also true of the
British study (7).
In both studies, the negative correlations with water hardness
or calcium ion seem to be stronger for 422 than for 420. If we
believe 420 to be a fairly homogeneous group, 422 would also have
to be accepted in the same way. And if so — what, then, is
the medical significance, the aetiology and the pathogenesis of
“other degenerative heart diseases”?
Summary
A study has been made on the relationship between deaths from
cardiovascular diseases and various parameters in drinking water
in 34 Swedish towns during 1951-60.
The figures indicate a highly significant negative correlation
between the calcium ion concentration and the statistical group
422 (“other degenerative heart diseases”).
Essentially the findings confirm results of similar studies
from other countries. It does also raise the problem of the
medical significance of the group 422.
Acknowledgements
We are indebted to the Swedish Association against Heart- and
Lung Diseases for financial support and to Statistiska
Centralbyrån for considerable aid in the statistical
analysis of the material.
References
1 CRAWFORD, M. D.: Personal communication 1964.
2. DINGLE, J. H., PAUL, O., SEBRELL, W. H., STRAIN,
W.H., WOLMAN, A. & WILSON, J. R.: Water composition and
cardiovascular health, Illinois Med. J. 125: 25, 1964.
3. GREENBERG, B. G.: Is soft water dangerous? J. Amer. Med.
Ass. 184: 85, 1963.
4. KEYS, A. & WHITE, P. D. ed.: Cardiovascular
epidemiology. Hoeber-Harper, New York 1956.
5. KOBAYASHI, J.: A geographical relationship between the
chemical nature of river water and death rate from apoplexy,
preliminary report. Ber. Ohara Inst. landw. Forsch.11: 12,
1957.
6. LINDEMAN, R. D. & ASSENZO, J. R.: Correlations between
water hardness and cardiovascular deaths in Oklahoma counties.
Amer.J. Publ. Hlth 54: 1071, 1964.
7. MORRIS, J. N., CRAWFORD, M. D. & HEADY, J. A.: Hardness
of local water supplies and mortality from cardiovascular disease
in the county boroughs of England and Wales. Lancet 1: 860,
1961.
8. MULCAHY, R.: The influence of water hardness and rainfall
on the incidence of cardiovascular and cerebrovascular mortality
in Ireland. J. Irish Med. Ass. 55: 17, l964.
9. MUSS, D. L.: Relationship between water quality and deaths
from cardiovascular disease. J. Amer. Water Works Ass. 54: 1371,
1962.
10. SAUER, H. I. & ENTERLINE, P. E.: Are geographic
variations in death rates from cardiovascular disease real? J.
Chron. Dis. 10: 513, 1959.
11. SAUER, H. I.: Epidemiology & cardiovascular mortality
— geographic and ethnic. Amer. J. Publ. Hlth 52: 94,
1962.
12. SCHROEDER, H. A.: Degenerative cardiovascular disease in
orient hypertension. J. Chron Dis. 8: 312, 1958.
13. SCHROEDER, H. A.: Relation between mortality from
cardiovascular disease and treated water supplies. J. Amer. Med.
An. 172: 1902, 1960.
14. SCHROEDER, H. A.: Relationship between hardness of water
and death rates from certain chronic degenerative diseases in the
U.S. J. Chron. Dis. 12: 586, 1960.
15. SCHROEDER, H. A.: Hardness of local water supplies and
mortality from cardiovascular disease. Lancet 1: 1171, 1961.
16. TURNER, R. C.: Radioactivity and hardness of drinking
waters in relation to cancer mortality rates. Brit. J. Cancer 16:
27, 1962.
Submitted for publication February 23, 1965.
This page was first uploaded to The Magnesium Web Site on July
18, 2001
http://www.mgwater.com/

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}