THE MAGNESIUM REPORT
CLINICAL, RESEARCH, AND LABORATORY NEWS FOR CARDIOLOGISTS
FIRST QUARTER 2000
Oral Magnesium and Wellness: Increased RDAs and Preventive
Medicine
RONALD J. ELIN, MD, PHD, AND ROBERT K. RUDE, MD
Traditionally, preventive medicine means elective stress
testing, mammography, screening for prostate-specific antigen,
and periodic lipid profiling. It also suggests an intent to be
proactive about lifestyle and behavior changes, including diet
and nutrient supplementation. Now we have evidence to add
adequate intake of magnesium—the "forgotten
electrolyte"—to our list of preventive health measures.
Ensuring adequate magnesium intake, either through dietary
sources of magnesium or the use of oral magnesium supplements,
constitutes a major step toward "wellness" that is justified by
scientific and clinical data. Both the graying of America and the
growing emphasis on exercise and fitness are reasons to take
extra care that magnesium intake is adequate. Suboptimal intake
of magnesium has been associated with a number of extremely
prevalent and potentially serious conditions. In addition, a
substantial portion of the American population is at risk for
chronic latent magnesium deficiency, which itself is a risk
factor for these and other conditions.
Why is chronic latent magnesium deficiency important, and what
can be done about it? For an answer, it is helpful to consider
the present Recommended Daily Allowance (RDA) of magnesium and
why it was increased.
1997 RDAs: The new standard
The RDA is the dietary intake that would provide an adequate
amount of a nutrient for nearly all the population. In practical
terms, this boils down to approximately 97% to 98% of the entire
population. RDAs are specific to life stages and gender.
Among the most potent reinforcements of the message that
magnesium is an essential nutrient for good health is the recent
endorsement of higher RDAs by the Institute of Medicine and the
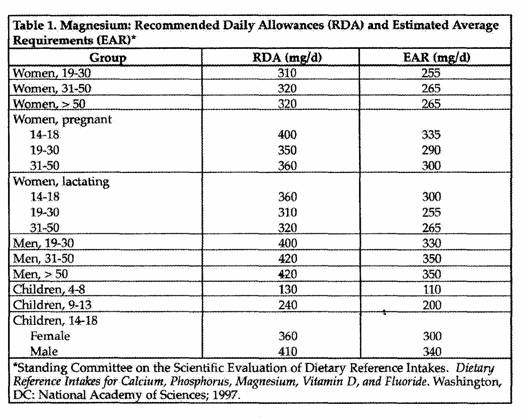
National Academy of Sciences. As of 1997, the RDA of magnesium
was raised 15%, to approximately 6 mg/kg/d. For men, this means
an increase from 350 mg/d to 420 mg/d, and for women from 280 mg
d to 320 mg/d (Table 1).
The National Academy of Sciences and the Institute of Medicine
reevaluate RDAs and their supporting data every decade. Review of
scientific information motivated the magnesium intake upgrade
promulgated by the Institute of Medicine in its 1997 Dietary
Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D,
and Fluoride. The experimental data on magnesium come from
dietary balance studies involving several different magnesium
intake levels under conditions in which diets were either
constant and controlled at clinical research centers or
self-selected in the community.
These studies, which were thought to provide a more accurate
and reliable estimate of dietary magnesium sufficiency involved
men and women of all ages—adolescence through older
adulthood. Magnesium content of foods was measured using atomic
absorption spectroscopy, and the study period was preceded by at
least a 12-day lead-in period to allow equilibration of magnesium
in the body. Earlier less accurate studies, in contrast, relied
on colonmetric methods for assessing magnesium content and
required, a lead-in period of as little as 2 days.
The estimated average requirement (EAR), on the other hand, is
the nutrient intake estimated to meet the need for a nutrient in
50% of the population. The EAR is among the factors on which the
RDA is based. While the EAR is determined from population
studies, the RDA is intended for advising individuals about
dietary needs. The current EAR corresponds to the previous (now
outdated) RDA 350 mg/d for men and 265 mg/d for women.
How Americans stack up
The upgrade in desired intake contrasts starkly to the reality
of population-based studies. Estimates suggest that between 50%
and 85% of the population of the United States is receiving an
inadequate magnesium intake. In a 1977-1978 study of almost
40,000 people, magnesium consumption met or exceeded the RDA
(which at that time was 5 mg/kg/d) in only 25% of those surveyed.
Many studies then showed that the average dietary intake in
adults ranged between 43.3% and 93.0% of that RDA, which was low
by present standards.
Today the proportion of individuals consuming their RDA of
magnesium remains low. Most people take in around 300
mg/d—estimates range from below 300 mg/d to around 325
mg/d. According to the US Department of Agricultures 1994
Continuing Survey of Food intakes by Individuals, the mean
magnesium intake by males age 9 and older was 323 mg/d— far
below today's RDA of 420 mg/d. Similarly, for women older than 9,
the mean intake was 228 mg/ d—again, significantly below
the RDA of 320 mg/d.
Intake decreases significantly in persons age 70 and
older—precisely those at highest risk for many of the
diseases associated with chronic latent magnesium deficiency.
Adolescent and adult women tend to take in suboptimal amounts of
dietary magnesium. Certain ethnic groups appear to have lower
magnesium intake than the general population. According to the
National Health and Nutrition Examination Survey (NHANES III)
from 1988 to 1991, magnesium intake is particularly low in
non-Hispanic blacks.
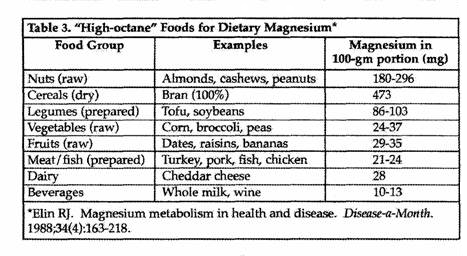
Changes in dietary habits and food preparation have
shortchanged us with respect to dietary magnesium. A century ago,
in the absence of processed foods, the average magnesium intake
exceeded 400 mg/d. Vegetarians, who eat mostly fresh foods of
plant origin still typically consume large amounts of magnesium.
As the nation's eating habits have gone from freshly prepared
items made in the home to prepared, processed meals and "fast
foods" taken on the run, the magnesium content of the food has
plummeted.
Refining and processing of grains and other foodstuffs
typically results in loss of 70% or more of the magnesium content
(as well as other nutrients). The conversion of wheat into flour
results in a loss of 82% of magnesium. Refining rice into
polished rice sacrifices 83% of the magnesium. Milling corn into
corn starch loses 98% of the magnesium. When soy beans are
cooked, they lose 69% of their magnesium. Quick-cooking oatmeal
provides only about 15% of the magnesium obtained from the
slow-cooking cereal.
The sodium and phosphate found in high amounts in many of
today's processed and prepared foods hinder the use of magnesium
in the body. A fast-food hamburger for example, packs a double
whammy; virtually devoid of magnesium itself, it is extremely
high in sodium, which facilitates magnesium loss. In addition,
phosphates and polyphosphates bind magnesium in the gut, leading
to magnesium malabsorption. Phosphates are found in soft drinks,
especially cola beverages (essentially devoid of nutritional
value), and polyphosphate preservatives are ubiquitous in baked
goods. The estimated average intake of phosphate is probably 2 to
3 times the RDA for a majority of the population—an
unfortunate reversal of the situation seen with magnesium that
aggravates the problem of chronic latent magnesium
deficiency.
All these data point to 2 reasonable conclusions. First the
American public consumes less magnesium than necessary for good
health. Second, magnesium supplementation, either in the form of
oral supplements or specific magnesium-rich foods may be of value
to many people, especially patients who have or are at risk for
many prevalent chronic diseases.
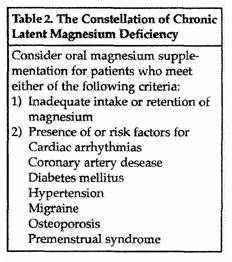
Chronic latent Mg deficiency
Chronic latent magnesium deficiency is the inadequate intake
or retention of magnesium in association with a constellation of
diseases (or risk factors for those diseases) in which magnesium
deficit is a risk factor or part of the pathophysiology. The
diseases and conditions for which risk is increased by chronic
but subclinical magnesium deficit include cardiac arrhythmias,
coronary artery disease (CAD), diabetes mellitus, hypertension,
migraine, osteoporosis, and premenstrual syndrome (Table 2).
Epidemiologic data from numerous clinical and population-based
studies have established links between inadequate magnesium
intake and elevated risk for cardiovascular diseases.
Longitudinal follow-up of more than 8,000 patients for 10 years
in the NHANES I Follow-up Study demonstrated inverse
relationships between total serum magnesium concentration and
risks of coronary heart and vascular disease deaths and
hospitalizations. Ascherio and colleagues found that blood
pressure tended to be lower in people whose fruit and vegetable
intake—and therefore magnesium intake—was high. In
the Honolulu Heart Study, the factor most strongly associated
with blood pressure control, was high magnesium intake. In the
Atherosclerosis Risk in Communities (ARIC) Study, involving more
than 15,000 participants, dietary magnesium intake was inversely
associated with systolic and diastolic blood pressures.
Lawrence M. Resnick, MD, of Cornell University Medical
College, has further outlined the strong link between magnesium
and hypertension in a previous issue of The Magnesium
Report (Resnick LR. Oral magnesium and hypertension:
Research and clinical application. The Magnesium Report.
1999; first quarter). Michael Shechter, MD, MA, of Tel Aviv
University, Israel, described his own successful research into
the use of oral magnesium to reduce risk of acute myocardial
infarction in patients with known CAD (Shechter M. Oral magnesium
in coronary artery disease: fresh insight on thrombus inhibition.
The Magnesium Report. 1999; August). Ezra A. Amsterdam,
M of the University of California, Davis, Medical Center
described the potential for event-rate reduction that oral
magnesium supplementation holds for patients at risk for cardiac
arrhythmias, including patients who have congestive heart
failure.
The connection between osteoporosis and magnesium is also
becoming stronger. Just last year, a subset analysis of the
Framingham Heart Study showed that dietary intake of magnesium
{as well as potassium) was directly related to bone mineral
density (BMD) and reduced declines in BMD in men and women. A
subset analysis of women who participated in the Aberdeen
Osteoporosis Screening Program suggested that high intakes of
magnesium and other electrolytes in milk and fruit over the long
term are associated with higher BMD and may be important to bone
health.
The common denominator between magnesium intake and these
diseases, as well as diabetes mellitus, migraine, and
premenstrual syndrome is chronic latent magnesium deficiency. It
is reasonable to suspect chronic latent magnesium deficiency in
any patient with cardiovascular disease, diabetes mellitus,
migraine, osteoporosis, or premenstrual syndrome, or risk factors
for any of these conditions. The approach for the clinician faced
with a patient in whom chronic latent magnesium deficiency is
suspected is to improve the dietary intake of magnesium and, if
necessary, provide oral magnesium supplementation (see Q&A:
Magnesium and Wellness). In a subsequent issue of The
Magnesium Report, chronic latent magnesium deficiency will
be described in greater detail and the practical aspects of the
relationship between magnesium intake and the diseases comprising
the constellation of chronic latent magnesium deficiency
including diabetes, will be discussed.
Suggested Reading
Ascherio A, Rimm PB, Giovannucci EL, et al. A prospective
study of nutritional factors and hypertension among US men.
Circulation. 1992; 86: 1475-1484.
Elin RJ. Magnesium metabolism in health and disease,
Disease-a-Month. 1988; 34: 161-218
Gartside PS, Glueck CJ. The important role of modifiable
dietary and behavioral characteristics in the causation and
prevention of coronary heart disease hospitalization and
mortality: the prospective NHANES I follow-up study. J Am
Coll Nutr. 1995; 14: 71-79
Joffres MR, Reed DM, Yano K. Relationship of magnesium intake
and other dietary factors to blood pressure: the Honolulu heart
study. Am J Clin Nutr. 1987; 45: 469-475
Ma J, Folsom AR, Melnick SL, et al. Associations of serum and
dietary magnesium with cardiovascular disease, hypertension,
diabetes, insulin, and carotid artery wall thickness: the ARIC
study. J Clin Epidemiol. 1995; 48: 927-940
New SA, Bolton-Smith C, Grubb DA, Reid DM. Nutritional
influences on bone mineral density: a cross-sectional study in
premenopausal women. Am J Clin Nutr, 1997; 65:
1831-1839.
Pan EM Mickle SJ. Problem nutrients in the United States.
Food Technology. 1981; 35(9): 58-69
Standing Committee on the Scientific Evaluation of Dietary
Reference Intakes. Dietary Reference Intakes for Calcium,
Phosphorus, Magnesium, Vitamin D, and Fluoride. Washington,
DC: National Academy of Sciences; 1997.
Tucker KL, Hannan MT, Chen H, Cupples LA, Wilson PWF, Kiel DP.
Potassium, magnesium, and fruit and vegetable intakes are
associated with greater bone mineral density in elderly men and
women. Am J Clin Nutr. 1999; 69 727-736.
The above article is from the "The Magnesium Report",
First Quarter 2000. Blaine Pharmaceuticals is the
manufacturer of Mag-Ox 400 and Uro-Mag magnesium
supplements.

Go to Blaine
Pharmaceuticals
Articles from "The Magnesium Report," a newsletter of
clinical, research, and laboratory news for
cardiologists, published by Blaine Pharmaceuticals
include:
- Oral Magnesium and
Hypertension: Research and Clinical Application,
Lawrence M. Resnick, MD.
- Oral Magnesium in Coronary Artery Disease: Fresh
Insight on Thrombus Inhibition, Michael Shechter, MD,
MA.
- Oral Magnesium for Cardiac Arrhythmias: Current
Clinical Perspective, Ezra A. Amsterdam, MD.
- Oral Magnesium and
Wellness: Increased RDAs and Preventive Medicine,
Ronald J. Elin, MD, PhD, and Robert K. Rude, MD.
- Medications, Alcohol
Consumption, and Magnesium: Ensuring Adequate
Intake of Oral Magnesium, Timothy J. Maher, PhD.
- Diabetes and Magnesium: The Emerging Role of Oral
Magnesium Supplementation, Jerry L. Nadler, MD.
|
This page was first uploaded to The Magnesium Web Site on
September 2, 2002
http://www.mgwater.com/
